
In
ancient medicine, the herb, Cannabis sativa L., was widely used to
cure disturbances and inflammation of the bowel. Research published
in the journal Pharmacology and by the United States (US) National
Institute of Health has found that cannabis is effective in treating
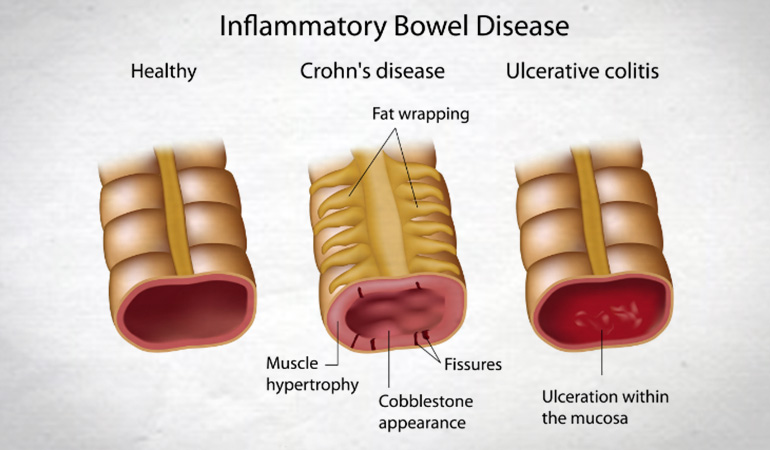
Crohn’s Disease, which is a form of inflammatory bowel disease
(IBD). IBD's such as Ulcerative Colitis and Crohn’s Disease affect
over a million people in the US. Many IBD victims suffer
from extreme pain, diarrhoea and poor ability to digest food. Up to
half of IBD cases are so severe that they ultimately require surgery
to remove the affected bowel segment.
In a 2007 study in Australia, The Economic Costs of Crohn’s Disease and Ulcerative Colitis, commissioned by Crohn’s and Colitis Australia (CCA) it was revealed that the (then) annual cost of Crohn’s Disease and Ulcerative Colitis was AU$2.7 billion. In 2013, CCA commissioned another report, Improving Inflammatory Bowel Disease Care Across Australia, which stated: "IBD is becoming more prevalent, more complex, and more severe ... IBD is a chronic and largely hidden disease affecting approximately 1 in 250 people aged 5 – 49 nationally. Australia has one of the highest rates of prevalence and incidence in the world and each year more and more young people are being diagnosed. Over 74,955 Australians are burdened with a constant and often hidden struggle that affects a sufferer’s personal, social and work life". The report went on to estimate that national total hospital costs for IBD are in the order of AU$100 million per annum. Productivity losses attributable to IBD in 2012 were estimated at over AU$380 million. An additional AU$2.7 billion of financial and economic costs have been associated with the management of IBD, Australia-wide.
In a 2007 study in Australia, The Economic Costs of Crohn’s Disease and Ulcerative Colitis, commissioned by Crohn’s and Colitis Australia (CCA) it was revealed that the (then) annual cost of Crohn’s Disease and Ulcerative Colitis was AU$2.7 billion. In 2013, CCA commissioned another report, Improving Inflammatory Bowel Disease Care Across Australia, which stated: "IBD is becoming more prevalent, more complex, and more severe ... IBD is a chronic and largely hidden disease affecting approximately 1 in 250 people aged 5 – 49 nationally. Australia has one of the highest rates of prevalence and incidence in the world and each year more and more young people are being diagnosed. Over 74,955 Australians are burdened with a constant and often hidden struggle that affects a sufferer’s personal, social and work life". The report went on to estimate that national total hospital costs for IBD are in the order of AU$100 million per annum. Productivity losses attributable to IBD in 2012 were estimated at over AU$380 million. An additional AU$2.7 billion of financial and economic costs have been associated with the management of IBD, Australia-wide.
The past decade has seen a constant rise in publications dealing with the anti-inflammatory effects of cannabinoids and the potential underlying mechanisms. Preclinical data on the ameliorating effect of synthetic and natural cannabinoids in animal models mimicking features of IBD have been rapidly evolving. The reasonable idea that cannabinoids would also be beneficial in IBD patients was mainly based on results from experiments in cannabinoid receptor knock-out mice and on data using cannabinoid receptor agonists and antagonists.
In 2011, a retrospective, observational study examining disease activity, use of medication, need for surgery and hospitalisation before and after cannabis use in 30 patients (26 males) with Crohn's Disease and a questionnaire performed by a different group of patients with Ulcerative Colitis (100) and Crohn's Disease (191), both revealed symptom relief and improvement after use of cannabis. 21 out of 30 of the study individuals reported significant improvement, with patients requiring steroid treatment reduced from 26 to 4.
 A prospective trial in Israel showed complete remission in five of eleven patients suffering Crohn's Disease who were given cannabis twice daily. Authors of the study said it had been reported for years that cannabis lessened the painful symptoms of the inflammatory bowel disease, but the findings had not been proven in a controlled trial. The study, published in Clinical Gastroenterology and Hepatology in 2013, compared 21 patients who did not respond to conventional treatment. Half were given cannabis cigarettes and the other half were given a placebo; cannabis cigarettes with the tetrahydrocannabinol (THC) removed. The results showed improvement in the group treated with the THC-intact cannabis. Those subjects also reported improved sleep and appetite.
A prospective trial in Israel showed complete remission in five of eleven patients suffering Crohn's Disease who were given cannabis twice daily. Authors of the study said it had been reported for years that cannabis lessened the painful symptoms of the inflammatory bowel disease, but the findings had not been proven in a controlled trial. The study, published in Clinical Gastroenterology and Hepatology in 2013, compared 21 patients who did not respond to conventional treatment. Half were given cannabis cigarettes and the other half were given a placebo; cannabis cigarettes with the tetrahydrocannabinol (THC) removed. The results showed improvement in the group treated with the THC-intact cannabis. Those subjects also reported improved sleep and appetite.The 8-week treatment with THC-rich cannabis caused a decrease in the Crohn's Disease activity index in 90% of patients without producing significant side effects. The mechanisms involved most likely include peripheral actions on cannabinoid receptors 1 and 2 (CB1 and CB2) and may also include central actions. The authors rightfully concluded that a larger patient group is warranted for future studies.

The wall of the gastrointestinal tract houses all components of the ECS. Data from 2011 showed that these components are differentially expressed in human IBD indicating a regulatory role in the disease progression. While anandamide and its synthesising enzyme display lower levels in Ulcerative Colitis, expression of CB2 receptors and enzymes responsible for synthesis and degradation of 2-AG were increased (from data in 2009). The findings indicate that the CB2 receptor plays a key role in the ameliorating effect of cannabinoids in IBD. The precise mechanism as to how cannabinoids contribute to the improvement of IBD, however, is not clear but by use of experimental models of intestinal inflammation we are able to define a picture on how and at which targets cannabinoids cause improvement of inflammation.
The primary mechanisms through which cannabis exhibits healing properties in Crohn's Disease are its immuno-modulatory and anti-inflammatory properties:

Natural and synthetic cannabinoids act via intestinal CB1 and CB2 receptors to regulate epithelial permeability, motility, secretion via the Enteric
Nervous System (ENS), as well as leukocyte migration, recruitment and apoptosis. As the site with the highest CB1 expression (but also some
CB2 expression), the brain may modulate motility, the sensation of pain and unpleasantness, thus positively influencing the inflammatory process.
In 2010, researchers at the University of Naples (Italy), released a study, Cannabinoids and the gut: new developments and emerging concepts, in which it was noted that cannabis was used to treat gastrointestinal conditions that ranged from enteric infections and inflammatory conditions to disorders of motility, emesis and abdominal pain. Anatomical, physiological and pharmacological studies have shown that the ECS is widely distributed throughout the gut, with regional variation and organ-specific actions. It is involved in the regulation of food intake, nausea and emesis, gastric secretion and gastro-protection, gastrointestinal motility, ion transport, visceral sensation, intestinal inflammation and cell proliferation in the gut. Cellular targets have been defined that include the Enteric Nervous System (ENS), epithelial and immune cells.
 |
| Figure 2 - The Organisation of the ENS of Human and Medium-Large Mammals |
It
should be emphasised that the brain is the major site of CB1
expression and that the presence of CB2 has also been detected in the
brain-stem. The use of cannabis in improving inflammation could
therefore well include central effects, such as a reduction in pain
sensation and relief of nausea and feeling of unpleasantness.



We should consider that other cannabinoids such as cannabidiol (CBD), cannabigerol (CBG) and tetrahydrocannabivarin (THCV), all of them non-psychotropic components of cannabis, have proven anti-inflammatory effects in experimental intestinal inflammation. Their actions should be regarded as additive beneficial effects of cannabis in the improvement of colitis in addition to THC-mediated effects.
There appears to be an established role for cannabis within gastroenterology for the following conditions: abdominal pain, anorexia, colitis, Crohn's Disease, diabetic gastroparesis (delayed gastric emptying), diarrhoea, emesis (vomiting), gastroenteritis and intestinal inflammation at the very least. The ancient use of cannabis in intestinal disturbances and over a decade of animal research, along with the above-mentioned human trials proves cannabis can treat and reduce the symptoms of patients with Crohn's Disease and a multitude of other gastrointestinal problems. Larger trials reiterating these results would go a long way to finally achieving broader acceptance of cannabis as a harmless and most efficacious medicine, and further trials to establish more about the involved mechanisms should reveal promising directions for future treatments.
No comments:
Post a Comment