Many different methods exist for testing for illicit drugs and the term ‘illicit drug’ can encompass a number of broad concepts, according to the Australian federal government they can include;
• illegal drugs; those prohibited from manufacture, sale or possession in Australia, for example, Cannabis, cocaine, heroin and ecstasy
• misuse, non-medical or extra-medical use of pharmaceuticals; drugs available from a pharmacy, over-the-counter or prescription, subject to misuse (opioid-based pain medications, opioid substitution therapies, benzodiazepines, over-the-counter codeine and steroids)
• other psychoactive substances; legal or illegal, used in a harmful way (kava, inhalants such as petrol, paint or glue [not tobacco or alcohol]).
Most employers, insurance companies, government agencies, etc., in the United States (US) and other jurisdictions, will ask for a urine test, the industry standard for workplace drug testing, and the only method approved for US federally mandated drug tests. A test for Cannabis is looking for a metabolite (chemical produced by the body from another chemical taken in by the body) of ∆9-tetrahydrocannabinol (THC), one of the main cannabinoids in the herb, Cannabis sativa L. Urine is used to test for the amount of just one of the metabolites of THC. The metabolite they are looking for in urine is THC COOH (carboxy-THC or 11-nor-∆9-tetrahydrocannabinol-9-carboxylic acid).
• illegal drugs; those prohibited from manufacture, sale or possession in Australia, for example, Cannabis, cocaine, heroin and ecstasy
• misuse, non-medical or extra-medical use of pharmaceuticals; drugs available from a pharmacy, over-the-counter or prescription, subject to misuse (opioid-based pain medications, opioid substitution therapies, benzodiazepines, over-the-counter codeine and steroids)
• other psychoactive substances; legal or illegal, used in a harmful way (kava, inhalants such as petrol, paint or glue [not tobacco or alcohol]).
Most employers, insurance companies, government agencies, etc., in the United States (US) and other jurisdictions, will ask for a urine test, the industry standard for workplace drug testing, and the only method approved for US federally mandated drug tests. A test for Cannabis is looking for a metabolite (chemical produced by the body from another chemical taken in by the body) of ∆9-tetrahydrocannabinol (THC), one of the main cannabinoids in the herb, Cannabis sativa L. Urine is used to test for the amount of just one of the metabolites of THC. The metabolite they are looking for in urine is THC COOH (carboxy-THC or 11-nor-∆9-tetrahydrocannabinol-9-carboxylic acid).
 THC is extensively metabolised to a number of substances including the active metabolite, 11-hydroxy-THC and the principal inactive metabolite, THC COOH. The active metabolite, 11-hydroxy-THC, is often cited as a marker of very recent Cannabis ingestion, as it is found at a higher concentration in blood when Cannabis is consumed rather than if smoked.
THC is extensively metabolised to a number of substances including the active metabolite, 11-hydroxy-THC and the principal inactive metabolite, THC COOH. The active metabolite, 11-hydroxy-THC, is often cited as a marker of very recent Cannabis ingestion, as it is found at a higher concentration in blood when Cannabis is consumed rather than if smoked. Although very small amounts of THC are excreted in urine, there is little value in attempting to identify it as it is only present for a short period following Cannabis use and testing requires a separate procedure. Urine testing for Cannabis involves firstly the detection of one or more cross-reacting cannabinoids using immuno-assay. Confirmation of Cannabis use involves the identification and often quantification of THC COOH using gas chromatography-mass spectrometry.
Although very small amounts of THC are excreted in urine, there is little value in attempting to identify it as it is only present for a short period following Cannabis use and testing requires a separate procedure. Urine testing for Cannabis involves firstly the detection of one or more cross-reacting cannabinoids using immuno-assay. Confirmation of Cannabis use involves the identification and often quantification of THC COOH using gas chromatography-mass spectrometry.
Of the estimated 55 million drug tests performed annually in the US, approximately 90% are urine tests. While often inaccurately referred to by employers and drug testers as an impairment test, urinalysis cannot detect the presence of any illicit drugs, including Cannabis, they can only identify the presence of non-psychoactive drug metabolites indicating a substance has been previously consumed at an unspecified point in time.
Unfortunately for Cannabis consumers, the primary metabolite THC-COOH is fat soluble and may remain detectable in urine for days and sometimes weeks after past use in regular partakers. Most standard urine tests can be easily influenced by dilution as most drug metabolites are water-soluble and are excreted rapidly from the body. However, THC-COOH is fat-soluble and exits the body slowly.
 It is difficult to say the length of time a person will test positive for Cannabis use since the metabolic process of the body converting THC into THC COOH can vary from person to person. While THC COOH has no psychoactive effects, it can be detected in urine for weeks, even months. It is not a marker for impairment, so it is arguably useless, but nevertheless, THC COOH has become the standard of evidence for determining if a person tests positive for Cannabis use. For infrequent Cannabis users, THC-COOH remains detectable in urine for several hours after one-time use; however, it’s commonly detectable on a standard urine screen for days or even weeks after past use in regular partakers.
It is difficult to say the length of time a person will test positive for Cannabis use since the metabolic process of the body converting THC into THC COOH can vary from person to person. While THC COOH has no psychoactive effects, it can be detected in urine for weeks, even months. It is not a marker for impairment, so it is arguably useless, but nevertheless, THC COOH has become the standard of evidence for determining if a person tests positive for Cannabis use. For infrequent Cannabis users, THC-COOH remains detectable in urine for several hours after one-time use; however, it’s commonly detectable on a standard urine screen for days or even weeks after past use in regular partakers.
Factors such as quantity consumed, frequency, method of consumption and even what food and drink is consumed can modify the amount of time that traces of THC COOH will be detectable in urine come test day. If it was just one night, would that make a difference? It depends as there are several studies that suggest a smaller “window of detection” (number of days following last use a urine sample will produce positive results) and others suggest a larger window, especially for chronic users.
Most agree, a one-time user is typically vulnerable to their urine testing positive for up to three days after use. After that, the chances of testing positive greatly decrease because any trace of THC COOH will likely fall below the required threshold for a positive result. The standard for most employment and US government testing programs is 50 nanograms per millilitres (ng/ml). It is possible, however, to test positive for over seven days. Frequent, regular Cannabis consumers should not be surprised to test positive for a minimum of one week to 10 days after their last use and up to 100 or more days thereafter.
Following Cannabis use via smoking, vaporising and other inhalation means, THC is rapidly absorbed and distributed into body fat. A 2001 study, 'The Forensic Pharmacology of Drugs of Abuse', out of the UK reported approximately 20% of THC is excreted in urine and 40% in faeces. THC is found in blood, oral fluid, hair and sweat; 11-hydroxy-THC is also found in blood, while THC COOH is the main urinary metabolite.
 In the body, THC is primarily metabolised in the liver where the hepatic cytochrome P450 enzyme oxidises THC to the active metabolite 11-hydroxy-Δ9-tetrahydrocannabinol (11-hydroxy-THC). This is then oxidised to the inactive 11-nor-Δ9-tetrahydrocannabinol-9-carboxylic acid (THC-COOH) and the conjugated THCCOOH-glucuronide. A number of other minor metabolites are also formed, including the active 8β-hydroxy-Δ9-THC and inactive 8α-hydroxy-Δ9-THC and 8α,11-dihydroxy-Δ9-THC. THC-COOH and 11-hydroxy-THC are most important for biological sample testing procedures.
In the body, THC is primarily metabolised in the liver where the hepatic cytochrome P450 enzyme oxidises THC to the active metabolite 11-hydroxy-Δ9-tetrahydrocannabinol (11-hydroxy-THC). This is then oxidised to the inactive 11-nor-Δ9-tetrahydrocannabinol-9-carboxylic acid (THC-COOH) and the conjugated THCCOOH-glucuronide. A number of other minor metabolites are also formed, including the active 8β-hydroxy-Δ9-THC and inactive 8α-hydroxy-Δ9-THC and 8α,11-dihydroxy-Δ9-THC. THC-COOH and 11-hydroxy-THC are most important for biological sample testing procedures.
Following Cannabis use via smoking, vaporising and other inhalation means, THC is rapidly absorbed and distributed into body fat. A 2001 study, 'The Forensic Pharmacology of Drugs of Abuse', out of the UK reported approximately 20% of THC is excreted in urine and 40% in faeces. THC is found in blood, oral fluid, hair and sweat; 11-hydroxy-THC is also found in blood, while THC COOH is the main urinary metabolite.

The question most often asked by clinicians, drug counsellors, lawyers and occupational health and safety representatives is, how long does Cannabis stay in the system? It is a reasonable question but one that cannot be answered in a few words. Firstly, most published studies on the excretion of Cannabis have been conducted using cigarettes containing a known amount of THC, either 1.75% or 3.55% and there is not necessarily a correlation between such controlled doses and use of 'street' Cannabis. Secondly, subjects are usually abstinent prior to the study and thirdly, there is a wide variability in excretion profiles between subjects.
The rate-limiting step in the metabolism of THC is the slow redistribution from body fat deposits into the blood. The concentration of THC found in fatty tissue becomes a function of the amount, frequency and potency of Cannabis smoked. Unlike interpretation of laboratory tests for the majority of 'drugs of abuse', Cannabis stands out as being the single substance that requires caveats before one can provide an interpretation; this being, was the person a naïve, occasional or chronic user? For naïve users, Cannabis can be eliminated within hours after use, usually within 24 hours.

In controlled studies in 1995, large inter-subject variability in the elimination of THC COOH, ranging from 8 hours in one subject and 1 day in three subjects was reported. In another study into occasional Cannabis use, volunteers who smoked a single THC cigarette once a week for 3 weeks determined an average elimination time of 2 days for cannabinoids.
Unfortunately there has been a paucity of data on the excretion and detectability of Cannabis in chronic users. Researchers advised that following use, urinary cannabinoids rise and then fall rapidly, taking up to 2 weeks in chronic users before dropping down to levels approaching the screening cutoff with reported levels of THC COOH sharply dropping to 20-50 ng/ml, and then decreasing at a much slower rate.
 Earlier studies on the elimination of Cannabis found residues of cannabinoids in subjects at up to 77 days of abstinence. However, they used a 20 ng/ml cutoff (cutoffs are simply reporting levels and a means of deeming whether a drug is present or not), not routine for urine testing. The most useful studies into the relationship between excretion patterns of cannabinoids and chronic users of Cannabis were conducted in the US up to 1998.
Earlier studies on the elimination of Cannabis found residues of cannabinoids in subjects at up to 77 days of abstinence. However, they used a 20 ng/ml cutoff (cutoffs are simply reporting levels and a means of deeming whether a drug is present or not), not routine for urine testing. The most useful studies into the relationship between excretion patterns of cannabinoids and chronic users of Cannabis were conducted in the US up to 1998.
These studies were predicated on an earlier finding which showed that by normalising the excreted amount of urinary THC COOH to the creatinine (Cannabis ratio), one obtained a more useful result. The best predictor of new use was achieved when the ratio was ≥ 0.5 relative to the previous sample taken at least 24 hours prior. In 2008 it was determined the elimination time in heavy Cannabis users correlated with the ratio in their first urination following abstinence.
Cutoffs were originally determined empirically, based on available technology. Today there is less of a relationship between the ability to detect a drug in a biological fluid and the cutoff. Originally, the screening cutoff for Cannabis was 20 ng/ml (1986); however laboratories were being challenged by claims of passive absorption, forcing the cutoff to be raised to 100 ng/ml. This resulted in fewer false positives but allowed many recent users to escape detection.

The screening cutoff is now accepted as 50 ng/ml (ug/l) and 15 ng/ml for the confirmatory analysis of THC COOH. Using a combination of 50 ng/ml screening cutoff followed by 15 ng/ml confirmatory cutoff, one obtained a confirmation rate of around 99%. Importantly, use of this combination eliminates any claims of passive inhalation. Interpretation of Cannabis results should always be predicated on the possibility of a negative gap, i.e., the time interval between first negative and last positive urine test.
As THC COOH is highly lipophilic (easily dissolved in fats) and re-absorption from fatty tissue is a slow process it can result in a negative urine occurring on one particular day followed by a positive test later. This negative gap is dependent on an individual’s body mass index (BMI). There is a direct correlation of BMI with the day of last positive urine; the higher the ratio at first urination, the longer the period between first negative and last positive urine. An initial low ratio implies low use and conversely, a high initial ratio confirms chronic use.

To date, the high individual variability in metabolism and excretion of cannabinoids precludes this approach, despite a number of research studies reporting various terminal elimination half-lives of THC COOH. Individual laboratory reports cannot be correlated with usage; however as more tests are conducted on individual patients or employees, the changing pattern of corrected metabolite becomes easier to interpret. In Australia, oral fluid testing for THC continues despite amendments to US workplace testing guidelines, recommending a moratorium on its use until the sensitivity of procedures becomes more robust.
Cannabis has been the most studied 'drug of abuse' due more to the prejudices of law-makers than any basis in science, and is the most prevalent illicit substance found in the workplace. Laboratory-based testing is a mature discipline with a high degree of accuracy. Interpretation of results remains contentious and as further studies evolve on the excretion by long-term users, it may be possible to use algorithms to accurately predict time of last use.
 In the US there are numerous products on the market that claim to cleanse the system or mask use. There are even some companies that offer 'clean' urine. There are many reasons to be doubtful of these products and their claims. Most do not work, are expensive and can even be identified in a drug test. Collection facilities and labs have become more sophisticated in detecting a specimen that has been influenced or altered.
In the US there are numerous products on the market that claim to cleanse the system or mask use. There are even some companies that offer 'clean' urine. There are many reasons to be doubtful of these products and their claims. Most do not work, are expensive and can even be identified in a drug test. Collection facilities and labs have become more sophisticated in detecting a specimen that has been influenced or altered.
There are, however, some simple, inexpensive and legal things that you can do to, purportedly, lower the amount of metabolites in your urine. Using one of many 100% guaranteed (in the US) safe detoxification products that naturally accelerate normal detoxification systems which allow you to cleanse your blood and urine of traces of Cannabis in roughly three to six days depending on many variables. And, never use the first urine of the day, typically referred to as 'the first void', even if you have to stay awake all night or get up early the day of the test, each time you urinate will make a difference. Also, try to avoid collecting the beginning of the urine stream, as this will have the greatest amount of metabolites in it.
 Flushing the system should be done with great caution as this involves putting large amounts of liquids (excluding alcoholic beverages) into the body so metabolites will be washed away faster. Although this may be an effective method, it can be dangerous. Ingesting too much water can cause water poisoning or water intoxication and can cause severe illness or even death. Cranberry juice is a natural diuretic and will help flush the system faster than water alone. Coffee and tea also act as diuretics. But, if urine is overly diluted it may raise a 'red flag'.
Flushing the system should be done with great caution as this involves putting large amounts of liquids (excluding alcoholic beverages) into the body so metabolites will be washed away faster. Although this may be an effective method, it can be dangerous. Ingesting too much water can cause water poisoning or water intoxication and can cause severe illness or even death. Cranberry juice is a natural diuretic and will help flush the system faster than water alone. Coffee and tea also act as diuretics. But, if urine is overly diluted it may raise a 'red flag'.
To enhance the colour of the urine (more yellow) you can add a Vitamin B tablet to your diet a day or two before the test. There is a lot wrong with urine drug testing, accuracy, privacy violations, proof that it improves workplace efficiency or safety. Unfortunately, until alternative methods are more widely available and accepted, it remains the go-to method in the US workplace.
Drug testing in Australia has been part and parcel of clinical management of patients on drug treatment programs since the late 1960's when methadone was introduced as a heroin substitute, wrote John H. Lewis Ph.D., in a 2009 bulletin, 'Clinical and medico-legal implications of drug testing for Cannabis', for the National Cannabis Prevention and Information Centre (NCPIC). The NCPIC is a consortium run under the auspices of the National Drug and Alcohol Research Centre Australia (NDARC), out of the University of New South Wales (UNSW), a federal Department of Health and Ageing initiative.
The NCPIC are Australia's self-proclaimed experts (leading, tax-payer and pHARMaceutical funded, 'reefer madness' mouthpiece for government propaganda) and Australia's equivalent to the US 'DARE' program. So it comes as no surprise that since then, the discipline has evolved into an industry encompassing public and private sector laboratories, forensic institutions and racing laboratories. The scope for drug testing has widened from clinical management to sport, the workplace, correctional institutions and the judicial system.
However, for many patients, especially those in residential rehabilitation environments, a policy of “no drugs” specifically includes Cannabis. In many drug treatment centres throughout NSW, concurrent use of Cannabis can adversely affect client management and there is now a deemed need for monitoring of the so-called 'Cannabis dependence'. Australian defence forces and many heavy industries maintain a strict drug policy and may dismiss personnel for continued Cannabis use.
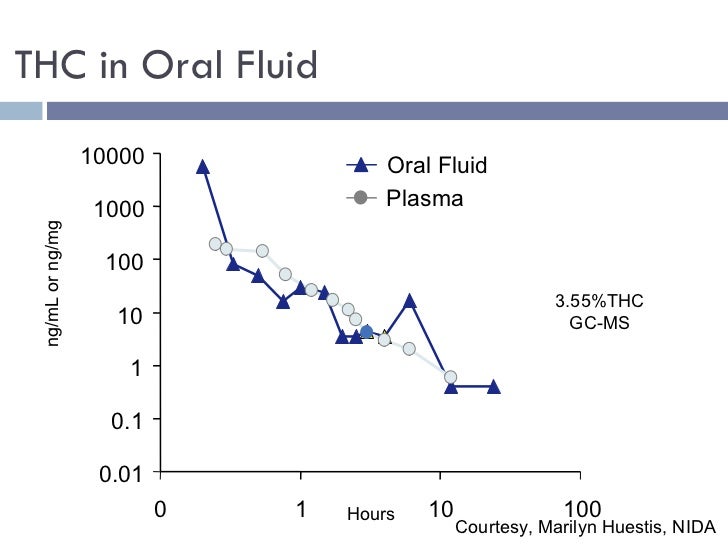
Although THC is found in saliva (or more correctly, oral fluid), levels are very low and there are often difficulties in recovery from collection pads. Essentially, THC comes from debris within the oral cavity after smoking, rather than diffusion from plasma. Studies in 2002 concluded for reliable identification of THC in oral fluid (fewest false negatives), the most appropriate screening cutoff should be set at 4 nanograms/millilitre (ng/ml), followed by a confirmatory cutoff of 2 ng/ml.
The ROSITA study (2001) concluded that no existing on-site device for THC was sensitive enough to be used for workplace drug testing. The issue at stake was one of duty of care. Studies such as ROSITA have been available for a number of years, yet many industries, wishing to avoid the often confrontational issues of mandating for urine tests, have opted for oral fluid testing.
Urine testing has the ability to identify infrequent as well as chronic Cannabis users and this may be perceived as either unfortunate, unfair or an invasion of their personal life outside the work environment. Conversely, current use of relatively insensitive on-site devices for saliva may be viewed as ineffective and to a degree, a failure to comply with a duty of care in eliminating risk of Cannabis-induced impairment in the workplace.

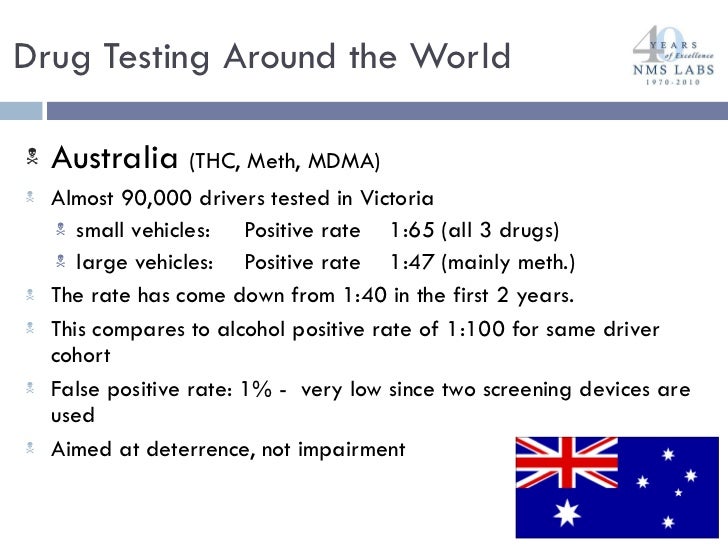
The Australian Drug Foundation, among other organisations across Australia, points out that saliva drug testing only tests for Cannabis, methamphetamines (ice) and ecstasy (MDMA). With detection time after last use for Cannabis being several hours upwards, based on potency, amount and individual metabolism. For ice and ecstasy, it is approximately 24 hours and detection times for opiates and benzo's are currently unknown. The current regime employed by Australian state law enforcement roadside (which is able to be used in the workplace) employs machines able to test for cocaine, opiates and some benzodiazepines (valium etc).
 According to Australian drug detection expert Tony Graham, incorporating a test for cocaine in the saliva swab would be a simple matter. "There is absolutely no reason, if they choose to, why they can’t do it", he said in November 2015. There is also absolutely no reason why police shouldn’t run sniffer dogs through places where bankers, lawyers and brokers are using cocaine, as well as where young people are using Cannabis!
According to Australian drug detection expert Tony Graham, incorporating a test for cocaine in the saliva swab would be a simple matter. "There is absolutely no reason, if they choose to, why they can’t do it", he said in November 2015. There is also absolutely no reason why police shouldn’t run sniffer dogs through places where bankers, lawyers and brokers are using cocaine, as well as where young people are using Cannabis!
It is not a road safety measure but an attack on lifestyles. It is hard otherwise to explain why some drivers are stopped more than once for ‘random’ tests, why the police were unwilling to comply with a Greens political party freedom of information request for the scientific basis of the tests, and why cocaine users are left out of the net.
 This is an expensive campaign. The drug test kits cost about $40 each and at last count there were five mobile drug testing buses in NSW alone, each costing up to $500,000. Add in the cost of training, laboratory work and all the television ads and it seems odd that the taxpayer should have to foot a bill of this size for activities that are not evidence based as Australian governments have lately found it hard to frame policies consistent with systematic knowledge, or even some science.
This is an expensive campaign. The drug test kits cost about $40 each and at last count there were five mobile drug testing buses in NSW alone, each costing up to $500,000. Add in the cost of training, laboratory work and all the television ads and it seems odd that the taxpayer should have to foot a bill of this size for activities that are not evidence based as Australian governments have lately found it hard to frame policies consistent with systematic knowledge, or even some science.
The Australian roadside drug test has defects that would trigger watchdog alarms were it not a government scheme. For a start it produces false positives. During ‘Operation Saturation’ (Northern Rivers, New South Wales, June to July 2015) tests were administered to 1,376 people. Of these, 246 returned positive results, but when immediately re-tested, 72 (more than a third) were found not to be positive at all. It misses the worst drugs and it penalises drivers who may be completely unaffected. The swabs test for Cannabis, amphetamine and ecstasy, but not opiates or pharmaceutical medications such as painkillers and anti-depressants, known to impair driving skills. They test for minuscule amounts of Cannabis, which means a trace amount in a driver’s body, perhaps days after ingestion, records a positive reading, even though there is no suggestion the Cannabis is affecting the driver.

The United Kingdom's March 2013 Wolff Report (expert panel looked at drug driving to establish world's best practice tests for drug impaired driving), 'Driving Under The Influence Of Drugs', found benzodiazepines, such as diazepam (valium [pharmacetical]) are the most common medicines detected in drivers involved in motor accidents and where the driver died in the accident; the second most commonly detected drug after alcohol. The report set a threshold level for impairment from diazepam at 550 micrograms per litre. This was halved when alcohol was present and they again recommended the blood alcohol limit be reduced to 0.02 when any benzodiazepine was also present.
In Australia, NSW Police have spent more than $6 million on roadside saliva drug testing kits they plan to use 100,000 times a year, only testing for ecstasy, Cannabis and amphetamines. Other states including Queensland, Victoria, Western Australia and the Northern Territory also perform roadside drug testing and police across the country at roadside tests are routinely waving through drivers who are highly medicated on prescription drugs that they don't even bother to check for. Some of these drivers will be on doses of drugs that are severely impairing their driving ability.
 |
| United Kingdom Wolff Report |
The Wolff report found benzodiazepines are the most common medicines detected in drivers involved in motor accidents and where the driver died in the accident, the second most commonly detected drug after alcohol. The report set a threshold level for impairment from diazepam at 550 micrograms per litre. This was halved when alcohol was present, and they again recommended the blood alcohol limit be reduced to 0.02 when any benzodiazepine was also present.
 The Wolff Report found Cannabis impairs driving at a blood concentration level of 5 micrograms per litre. Because Cannabis and alcohol interact to increase impairment they also found when both substances are present the safe level of Cannabis reduces to 3 micrograms per litre. The safe level of alcohol also reduces when in combination with Cannabis from a blood alcohol level of 0.05 to 0.02.
The Wolff Report found Cannabis impairs driving at a blood concentration level of 5 micrograms per litre. Because Cannabis and alcohol interact to increase impairment they also found when both substances are present the safe level of Cannabis reduces to 3 micrograms per litre. The safe level of alcohol also reduces when in combination with Cannabis from a blood alcohol level of 0.05 to 0.02. The report went through this same process for pretty much every commonly known drug from ecstasy to heroin, amphetamines to morphine. It used peer-reviewed scientific papers and epidemiological studies to set rational limits for the presence of drugs that directly relate to driver impairment. It applied evidence and rational thought to a difficult social problem and in doing so it came up with a sensible solution that squarely addressed driver safety. Of course this is the exact opposite of what we have in NSW and right across Australia, where ideology and a failed 'zero tolerance' approach to a handful of illegal drugs is seriously skewing the police effort.
The report went through this same process for pretty much every commonly known drug from ecstasy to heroin, amphetamines to morphine. It used peer-reviewed scientific papers and epidemiological studies to set rational limits for the presence of drugs that directly relate to driver impairment. It applied evidence and rational thought to a difficult social problem and in doing so it came up with a sensible solution that squarely addressed driver safety. Of course this is the exact opposite of what we have in NSW and right across Australia, where ideology and a failed 'zero tolerance' approach to a handful of illegal drugs is seriously skewing the police effort.
It would be a safe bet that most if not all of the convictions recorded against drivers in NSW and across other Australian jurisdictions from random tests concerned levels much lower. The Wolff Report also tabulates the driving impairment thresholds of other drugs, including combinations of drugs with alcohol and finds the most dangerous to be the valium-type medications.
Such prescription drugs are the most often detected in drivers involved in accidents and the second most likely (after alcohol) to be found where the motorist died in the accident. Why has our legislation ignored scientific evidence? Probably because mobile drug testing originated in Victoria in 2004 when there was less evidence available (the Wolff Report came out in March 2013). Other states have adopted the Victorian model (and the drug kits that are manufactured in Victoria) without, apparently, giving it any critical thought.

Another reason for avoiding evidence-based legislation is less benign. Right-wing ‘war on drugs’ ideologues are keen to use the police in their attacks on unruly minorities. Ironically, some parts of government are beginning to see the benefits of medicinal Cannabis. The cultural warriors bitterly resist this development, which blurs the simple black-and-white, them-and-us dichotomy they operate under.
World’s best practice would abandon the ideology of the war on drugs in favour of measures for genuine road safety. It would give us tests that can identify all the drugs of concern, tests that do not produce numerous false positives and tests that measure the actual driving impairment of those being tested. Until random drug tests achieve that minimum level of practicality and justice, the public should be wary of the motives of the politicians pushing them.
World’s best practice would abandon the ideology of the war on drugs in favour of measures for genuine road safety. It would give us tests that can identify all the drugs of concern, tests that do not produce numerous false positives and tests that measure the actual driving impairment of those being tested. Until random drug tests achieve that minimum level of practicality and justice, the public should be wary of the motives of the politicians pushing them.
New South Wales defence lawyer Steve Bolt suggested a line of defence to Cannabis users in early 2016. He offered that drivers in New South Wales should visit the Centre For Road Safety's web page, 'Drugs and Driving', and read the section that states, "Cannabis can typically be detected in saliva by an MDT test stick for up to 12 hours after use". They added the word 'typically' the day after the Police v Joseph Carrall case in Lismore when the Magistrate acquitted the driver for relying on the advice of police that he would be fine to drive within a certain time frame, and he wasn't.
"If you therefore wait at least 12 hours after using Cannabis you can reasonably expect it will not be detected, according to advice provided by the NSW government. A precedent has been set which could allow you to test this in court. The onus is on the prosecution to prove otherwise". But there is no guaranteed outcome as ultimately it is up to the Magistrate.
In drug testing in Australia, two standards are used as the basis:
- AS/NZS 4308:2008 Procedures for specimen collection and the detection and quantitation of drugs of abuse in urine
- AS 4760:2006 Procedures for specimen collection and the detection and quantitation of drugs of abuse in oral fluid
The steps in a drug testing process are:
- sample collection;
- screening test;
- confirmatory testing.
The reliability of the result may be compromised by any of these steps not being performed properly. For example, a well performed test will never compensate for a poorly acquired or badly managed sample.
In July 2013 accreditation of on-site drug testing of oral fluid (AS 4760, Section 3) was suspended by the National Association of Testing Authorities (NATA) due to significant technical issues with the standard. NATA accreditation is a means of providing everyone with confidence in the competence of drug testing services through its third-party, peer assessment processes.
In January 2016 Technical Annex 1, in regard to AS 4760 Section 3 On-site Initial Testing, stated; “Having conducted several assessments, it has become apparent that there are a number of significant issues with Section 3 of AS 4760:2006 which remain unable to be resolved. This is despite NATA seeking independent feedback to clarify these issues from key professional bodies including the Royal College of Pathologists of Australasia (RCPA), the Australasian Association of Clinical Biochemists (AACB) and from our counterpart organisation in New Zealand, International Accreditation New Zealand (IANZ). Accordingly, NATA has not granted accreditation to any facility for AS 4760, Section 3 and a decision has now been made to withdraw the provision of accreditation for this testing. A communication to this effect was sent to NATA's stakeholders in July 2013. Until further notice NATA will no longer accept applications for accreditation in this area and any current applications will no longer be progressed”.
The issues identified in relation to this testing include the following:
- There are no prescribed cut-off concentrations for screening devices or set quality control limits as there are for urine screening devices as detailed in Appendix A of AS/NZS 4308:2008.
- The target concentrations for screening devices ... are described as “nominated” in Section 1.5. This Section also states that “there is yet to be an accepted cut-off concentration” and that “concentrations higher than the initial testing target concentrations may sometimes be used if sensitivity is the limiting factor but this reduces the ability to detect drug use”. Accordingly, a facility may nominate its own targets (but not lower than those used for confirmatory testing). Where the nominated targets are set higher ... by the facility due to the insensitivity of a screening device, false negative results may result, despite compliance with the Standard. This would be a key concern for both drug screening programs and the public.
- The ability to test for drugs with known instability in saliva post collection, especially tetrahydrocannabinol (THC), is compounded by the allowance of “nominated” targets. The allowance of nominated screening concentrations at levels at or above the confirmatory concentrations may impact on the ability of confirmatory testing to reproduce a non-negative screening result due to loss of drug during transport and handling.
- There are no acceptance criteria for what constitutes acceptable verification of screening devices as there are for urine screening devices as detailed published in Appendix B of AS/NZS 4308:2008.
- The Standard requires quality control (QC) to be run. However, it is noted that the negative QC is defined as a drug free specimen. Such a specimen does not test the sensitivity of a device to identify donor samples which contain drugs at a concentration below the nominated target cut-offs. This is inconsistent with Appendix A of AS/NZS 4308:2008 which requires the below cut-off QC to be at a concentration between 25-50% below the cut-off concentration. The positive control is at or within 50% above the nominated concentrations. This is also inconsistent with AS/NZS 4308:2008 which requires the positive control to be between 25-50% above the cut-off concentrations.
“Whilst NATA will not consider granting accreditation for testing to AS 4760:2006, Section 3, agencies are still testing and claiming compliance with the Standard. It is NATA's view that this poses a significant risk to health and safety given the deficiencies as noted above”.

The best way to deal with Cannabis on the roads in Australia is to legalise, and to gauge the effect Cannabis legalisation can have on the roads, we need only look at what has happened since legalisation took effect in Colorado, US. A month-by-month comparison of highway fatalities in Colorado through half of 2015 and 2014 along with highest fatality figures for each month since 2002, the lowest for each month since 2002 and the average for each month since 2002. If Australian governments were serious about reducing deaths on the roads they would stop doing the same things over and over and expecting different results. We all know that is the definition of insanity. Let's reduce the road carnage, dispense with testing for Cannabis and relegalise it!
The best way to deal with Cannabis on the roads in Australia is to legalise, and to gauge the effect Cannabis legalisation can have on the roads, we need only look at what has happened since legalisation took effect in Colorado, US. A month-by-month comparison of highway fatalities in Colorado through half of 2015 and 2014 along with highest fatality figures for each month since 2002, the lowest for each month since 2002 and the average for each month since 2002. If Australian governments were serious about reducing deaths on the roads they would stop doing the same things over and over and expecting different results. We all know that is the definition of insanity. Let's reduce the road carnage, dispense with testing for Cannabis and relegalise it!
*Cannabis - Cannabis sativa L. is a member of the Cannabaceae family. Cannabis is the plant genus, sativa (Latin for 'cultivated') is the species (in many plant species names, e.g., rice is Oryza sativa L.), and the 'L.' (not always used) denotes the authority who first named the species, Carolus (Carl) Linnaeus, the Swiss botanist considered the 'Father of Taxonomy'. Cannabis sativa L., is; an annual, herbaceous - denoting or relating to herbs (in the botanical sense), usually dioecious - either exclusively male or exclusively female, or monoecious - having the stamen (male, pollen-containing anther and filament) and the pistil (female, ovule-bearing) in the same plant (hermaphrodite). Thus, as the Help End Marijuana Prohibition (HEMP) Party of Australia so rightly point out, Cannabis is a herb!
Adapted from; Standards AU Presentation Dec 2013, Drug Screening Products-Services, How Long Does THC Stay In Your System, Drug Testing, Safer Behaviours - Drug Driving FAQs, Bulletin 7 Clinical and Medico-legal Implications of Drug Testing for Cannabis, Roadside Drug Testing The Magic 12 hour Rule, Human Cannabinoid Pharmacokinetics, Roadside Drug Testing Shouldn't Ignore The Commonly Used Drugs, Cannabinoid Concentrations in Spot Serum Samples 24-48 Hours After Discontinuation of Cannabis Smoking, Urinary Excretion Profiles of 11-nor-9-carboxy-∆9-tetrahydrocannabinol and 11-hydroxy-∆9-THC, Tolerance and Disposition of Tetrahydrocannabinol in Man, Differentiating New Marijuana Use From Residual Drug Excretion in Occasional Marijuana Users, Urinary Elimination of 11-nor-9-∆9-tetrahydrocannabinol in Cannabis Users During Continuously Monitored Abstinence, Oral Fluid Testing For Drugs of Abuse ..., ROSITA Roadside Testing Assessment, Drug Driving Law Fails Justice Test, The ABCs of Marijuana and Drug Testing, Detecting and Quantifying THC In Oral Fluids, Developments in Toxicology, Information Paper 10 - Workplace Drug Testing - a Guide to Industry
No comments:
Post a Comment